"Generic 20 mg torsemide with amex, blood pressure medication breastfeeding".
Q. Vigo, M.B. B.A.O., M.B.B.Ch., Ph.D.
Program Director, Des Moines University College of Osteopathic Medicine
The mechanism of therapy is thought to be the same as ipilimumab pulse pressure 83 20 mg torsemide cheap otc, with non-specific autoimmune effects heart attack ukulele 10 mg torsemide generic free shipping. Checkpoint inhibitors may have clinical application in head and neck cancer due to the general mechanism of releasing immune inhibition heart attack alley torsemide 10 mg order online. An objective response was seen in between 6 to 17% of patients, and stabilization of disease in 12 to 41% of patients. Ruxolitinib has been shown to be clinically effective in myeloproliferative neoplasms as well as rheumatic conditions. Cytokines are another small molecular adjuvant therapy that has been used both alone and in combination with other immunotherapies. In advanced head and neck cancer, eight patients were enrolled to receive infusion of interferongamma resulting in three measurable responses and four patients with stable disease. There has been little work with this agent in head and neck cancer since that study. The two deaths (multiorgan failure and subarachnoid hemorrhage) were not considered related to the study drug. Subsequent downstream signaling activates antigen presenting cells and initiate a Th1 response. Four weeks after therapy 35% of patients were complete responders and 46% were partial responders, and all complete responses were durable over time. There are preclinical data in a rat model of oral dysplasia that demonstrated regression of mild dysplasia or hyperplasia and in one case the regression of a well differentiated squamous cell carcinoma lesion. Most p53 mutations result in the accumulation of p53, therefore non-mutated portions of the protein are susceptible to degradation into wild type (wt) peptide sequences appropriate for immune presentation. A phase I trial examining p53 multiple-peptide/dendritic cell vaccine in head and neck cancer patients (University of Pittsburgh) was reported on in a 2009 abstract. Patients treated for advanced head and neck cancer, with no active disease, were vaccinated with (wt) p53 sequences pre-loaded onto autologous dendritic cells. At 15-month follow up, 11 of 16 patients were alive without disease and two patients had recurrent disease. All patients had vaccine induced T cell responses; and, at 12 months, 15 out of 19 patients had clinical responses and nine had complete responses). Seventeen of these patients with advanced head and neck cancer went on to receive post-treatment neck dissection. This strategy avoids some of the limitations of in vivo T cell expansion with other immunotherapeutic approaches that are impacted by either local or systemic tumor-associated immunosuppression. The re-injection of tumorspecific T-cells has resulted in long-term, durable responses in some patient populations with advanced tumors. This is an extremely labor intensive method in which dendritic cells are isolated from each patient, and they are loaded with tumor antigen ex vivo. Often the tumor cells are given with adjuvant agents or modified by viral infection to improve their immunogenicity. These vaccines tend to be labor intensive because the tumor has to be isolated and processed before it can be used as a 4308 vaccine. It is unlikely that a drug-based strategy alone will destroy all cancer cells in patients with advanced epithelial malignancies. While tumor-eradicating immunity can be achieved in a small number of patients, the key will be to understand how to achieve similar results in a larger population of patients. Protective mechanisms of head and neck squamous cell carcinomas from immune assault. The activation of natural killer cell effector functions by cetuximab-coated, epidermal growth factor receptor positive tumor cells is enhanced by cytokines. Immune activation by epidermal growth factor receptor specific monoclonal antibody therapy for head and neck cancer. Immune escape associated with functional defects in antigen-processing machinery in head and neck cancer. Human leukocyte antigen class I allelic and haplotype loss in squamous cell carcinoma of the head and neck: clinical and immunogenetic consequences. Investigation of interleukin 10, 12 and 18 levels in patients with head and neck cancer. Overexpression of transforming growth factor beta1 in head and neck epithelia results in inflammation, angiogenesis, and epithelial hyperproliferation.
Diseases
- Dentin dysplasia, radicular
- Fucosidosis type 1
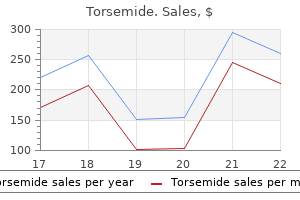
- Essential hypertension
- Hypoparathyroidism X linked
- Vein of Galen aneurysmal malformationss (VGAM)
- Microinfarct
- Porokeratosis of Mibelli
- Warkany syndrome
- Granulomas, congenital cerebral
Postoperative or postintubation care includes the need for frequent suctioning and high air humidity to maintain airway or endotracheal tube patency prehypertension values order torsemide 20 mg fast delivery. Intravenous antibiotic treatment has traditionally included a third-generation cephalosporin such as cefotaxime or ceftriaxone in combination with a penicillinase-resistant penicillin such as oxacillin or nafcillin heart attack remixes torsemide 10 mg order mastercard. A temporary tracheostomy is a consideration if the child with bacterial tracheitis fails extubation or if intubation is prolonged despite appropriate medical management arrhythmia usmle 20 mg torsemide purchase otc. The goals in such patients are to avoid intubation trauma and subsequent stenosis of the inflamed tracheal mucosa as well as improve pulmonary toilet. Characterized by paroxysmal coughing and named for the classic inspiratory "whooping" sound at the end of the cough, pertussis was the leading cause of infant mortality in the prevaccination era. Transmission occurs via aerosolized droplets produced by the cough of infected individuals, attaching to and damaging ciliated respiratory epithelium. In response, an exudate forms in the respiratory passageways occluding the smaller airways, especially in infants and small children, leading to atelectasis, cough, cyanosis and pneumonia. Prognosis is now excellent, and complications are usually minimal, with most patients making a gradual recovery with supportive care. Vaccination from whole Bordetella pertussis was available (combined with diphtheria and tetanus) from the 1940s through the 1990s but was associated with adverse effects. Symptoms include sore throat, hoarseness and fever, followed by progressive airway obstruction. Since the introduction of the diphtheria toxoid in the 1920s, the disease has been well controlled. With immunization, only about 1000 cases are reported annually in the United States. Those at risk to contract the illness include children whose immunization status is incomplete. This group includes those who are immunocompromised, were never immunized, received an inefficient immunization or had an inadequate response to immunization, and those not receiving a booster after previous immunization. The microorganism causes an inflammatory response in the mucous membranes resulting in a thick, tenacious, gray exudative plaque that coats the upper and lower respiratory tract and bleeds upon attempted removal. Diagnosis is based on these classical clinical examination findings and confirming cultures. Treatment requires establishing a safe airway, often via tracheostomy, and administering both diphtheria anti-toxins (toxoid) and antibiotics (penicillin or erythromycin). Examples of vocal abuse include yelling or shouting, chronic throat clearing and coughing, with the former being the most common cause in children presenting with hoarseness. Other causes of traumatic laryngitis are iatrogenic injury, muscle tension dysphonia and thermal/chemical inhalational injuries. These insults may result in hemorrhage or edema at the microscopic level on the mucosal surface of the true-vocal folds or within Reinke space. If the phonotrauma is of short duration, the process is usually self-limited, requiring only correction of the offending behavior. Voice rest and humidification, as well 3179 as initiation of antireflux medications, are the typical first-line treatments. Such nodules are very common in children and tend to resolve once the child learns to modulate their voice better. In older children who may be more motivated to improve their vocal quality due to peer pressure, voice therapy may be of some benefit. Intubation can lead to injury to the larynx as well with secondary nonspecific granuloma formation. Granulomas are benign unilateral or bilateral lesions most commonly located on the vocal folds at the vocal processes of the arytenoid catilages. Histologically, they resemble pyogenic granulomas consisting of chronic inflammatory infiltration with neovascularization and fibrosis covered by squamous-cell epithelium. Once the inciting agent, the endotracheal tube, is removed, the granulomas will often resolve. However, in some circumstances, the granulation tissue resolves incompletely or matures into chronic laryngeal scarring. Patients with intubation granulomas may present weeks to months after extubation with voice change, globus sensation or, rarely, airway obstructive symptoms. Treatment consists of empirical protonpump inhibitor therapy and, if the granuloma does not resolve or is causing obstructive symptoms, removal via microscopic direct laryngoscopy. A granuloma is an imprecise term for any small, nodular, poorly 3180 demarcated aggregation of mononuclear inflammatory cells.
Altered absorption or metabolism of thiamine hypertension juice recipe purchase 20 mg torsemide mastercard, folic acid arteria3d pack unity torsemide 20 mg buy line, pyridoxine blood pressure kiosk machines buy torsemide 10 mg mastercard, vitamin A, vitamin B12, sodium, potassium, magnesium, calcium, phosphorus, zinc, and selenium can result. Long-term alcoholism can also induce hepatic cirrhosis, with the potential development of ascites and/or hepatic encephalopathy. Glucose intolerance may be observed in alcoholics secondary to pancreatic inflammation or injury. Table 107-4Physical Findings and Associated Nutrient Deficiencies/Excesses Finding Deficiency Excess Hair and nails 4325 Transverse hair depigmentation Protein Sparse hair Protein, biotin, zinc Vitamin A Corkscrew hair Vitamin C Transverse nail ridging Protein Skin Scaling Vitamin A, zinc, fatty acids Vitamin A Cellophane appearance Protein Cracking dermatitis Protein Follicular hyperkeratosis Vitamins A, C Petechiae Vitamin C Purpura Vitamins C, K Pigmentation, desquamation of sun-exposed areas Niacin Yellow sclerae pigmentation-sparing Carotene Eyes Papilledema Vitamin A Night blindness Vitamin A Perioral 4326 Angular stomatitis Riboflavin, pyridoxine, niacin Cheilosis Riboflavin, pyridoxine, niacin Oral Atrophic lingual papillae Riboflavin, niacin, folate, vitamin B12, protein, iron Glossitis Riboflavin, niacin, folate, vitamin B12 pyridoxine, Hypogeusia, hyposmia Zinc Swollen, gingiva retracted, bleeding Vitamin C Neurologic Headache Vitamin A Drowsiness, lethargy, vomiting Vitamins A, D Dementia Niacin, vitamin B12, folate Confabulation, disorientation Thiamin Ophthalmoplegia Thiamin, phosphorus Peripheral neuropathy Thiamin, pyridoxine, vitaminB12 Pyridoxine Tetany Calcium, magnesium Others 4327 Parotid enlargement Protein (consider bulimia) Heart failure Thiamin, phosphorus Hepatomegaly Protein Vitamin A Edema Protein, thiamin Poor wound healing, decubitus ulcers Protein, vitamin C, zinc Commonly used methods for obtaining a dietary history include the 24-hour recall, a one to seven day food intake record, and a food frequency questionnaire. A number of computer programs allow rapid estimation of nutrient intake based on these records or questionnaires. It is important to remember that in the course of the complete medical history, information elicited from the patient in all of the areas noted in Table 107-6 will aid in identifying possible nutrient deficits not gathered from the dietary recall. The Karnofsky performance status is a scoring system commonly used to assess functional status. It is useful as a predictor of therapy-related decline in nutritional status and is a helpful addition to the comprehensive assessment. The lower end of the calorie range should be the initial calorie goal if a patient is at re-feeding risk. If gradual weight gain or nutritional repletion is the aim, 250 to 500 kcals/day is added to total maintenance calorie need. Protein Needs Acceleration in protein turnover and derangements in protein metabolism have been observed in patients with cancer. In contrast to simple starvation, protein use increases when a patient with cancer is under metabolic stress. Protein needs are usually calculated based on actual weight or adjusted weight for obesity. The approximate protein need can be adjusted based on the degree of protein depletion and metabolic stress factors. If a patient with head and neck cancer undergoes a large operation with reconstruction, protein needs for healing may be up to 2. The amount of protein need calculated, or provided, may require adjustments if renal or liver disease is present. Table 107-6Nutrition History Survey Mechanism of Deficiency History Deficiency to Suspect Inadequate intake Alcoholism Calories, protein, thiamin, niacin, folate, pyridoxine, riboflavin Avoidance of vegetables, grains fruit, Vitamin C, thiamin, niacin, folate Avoidance of meat, dairy products, eggs Protein, vitamin B12 Constipation, hemorrhoids, diverticulosis Dietary fiber 4330 Isolation, poverty, disease, idiosyncrasies dental food Various nutrients Weight loss Calories, other nutrients Inadequate absorption Drugs (especially antacids, anticonvulsants, cholestyramine, laxatives, neomycin, alcohol) Varies, dependent on drug Malabsorption (diarrhea, weight loss, steatorrhea) Vitamins A, D, and K; calories; protein; calcium; magnesium; zinc Parasites Iron, vitamin tapeworm) B12 (fish Pernicious anemia Vitamin B12 Surgery (Gastrectomy, intestinal resection) Vitamin B12 (if distal ileum), iron, others as in malabsorption Decreased utilization Drugs anticonvulsants, antimetabolites, contraceptives, alcohol) (especially oral isoniazid, Varies, dependent on drug Inborn errors of metabolism (by family history) Various nutrients Increased losses Alcohol abuse Magnesium, zinc Blood loss Iron Paracentesis (ascitic, pleural) Protein 4331 Diabetes, uncontrolled Calories Diarrhea Protein, zinc, electrolytes Draining abscesses, wounds Protein, zinc Nephrotic syndrome Protein, zinc Peritoneal dialysis hemodialysis or Protein, water-soluble vitamins, zinc Increased requirements Fever Calories Hyperthyroidism Calories Physiologic demands (infancy, adolescence, pregnancy, lactation) Various nutrients Surgery, trauma, infection burns, Calories, protein, vitamin C, zinc Tissue hypoxia Calories utilization) (inefficient Cigarette smoking Vitamin C, folate the best method for determining if protein needs are being met is by monitoring for gradual weight gain and positive nitrogen balance. Measurement of nitrogen balance is most accurate in those patients where intake can be quantified definitively, as with enteral or parenteral nutrition. Accurate measurement remains challenging and requires cumbersome 24-hour urine collection. Urine-nitrogen losses can further be affected by critical illness and fluctuations in renal function. For these patients, nitrogen balance is more accurately estimated using urea kinetics. Observing a patient for signs and symptoms of deficiency Table 107-4) can help determine the need for vitamin and/or mineral supplementation. In addition, supplementation may be considered in patients with high risk of re-feeding syndrome, history of alcohol abuse, poor diet quality, and need for healing. Zinc deficiency is fairly common in the head and neck cancer population, with 4333 approximately 50% having deficiency at baseline. It has been suggested that zinc supplementation aids in decreasing the impact of radiation therapy on taste. The use of multivitamins and mineral supplements during cancer treatments is an area of debate. In theory, antioxidant supplementation may interfere with the desired effect from free radical generation during adjuvant therapy, hindering treatment efficacy. A lycopene-rich diet appeared to be protective against oropharyngeal cancer development in a case-control study.